三阶四维5D,让创新策源“最先一公里”火起来
开云网页登录 第十届校史演讲大赛火热报名中
开云网页登录 崇明校区项目启动
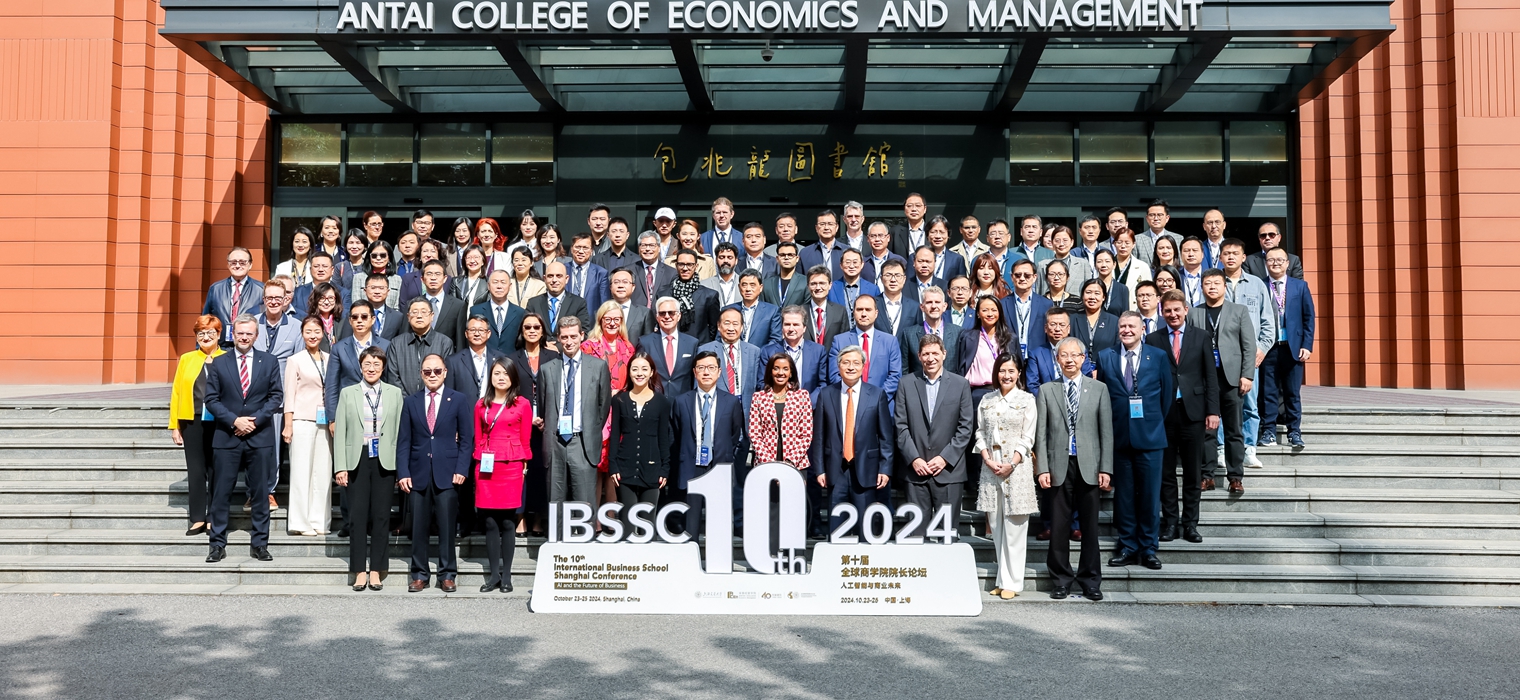
第十届全球商学院院长论坛在开云网页登录 举办
开云app官网入口下载苹果版 原创“大师剧”《海菜花开》再度盛放
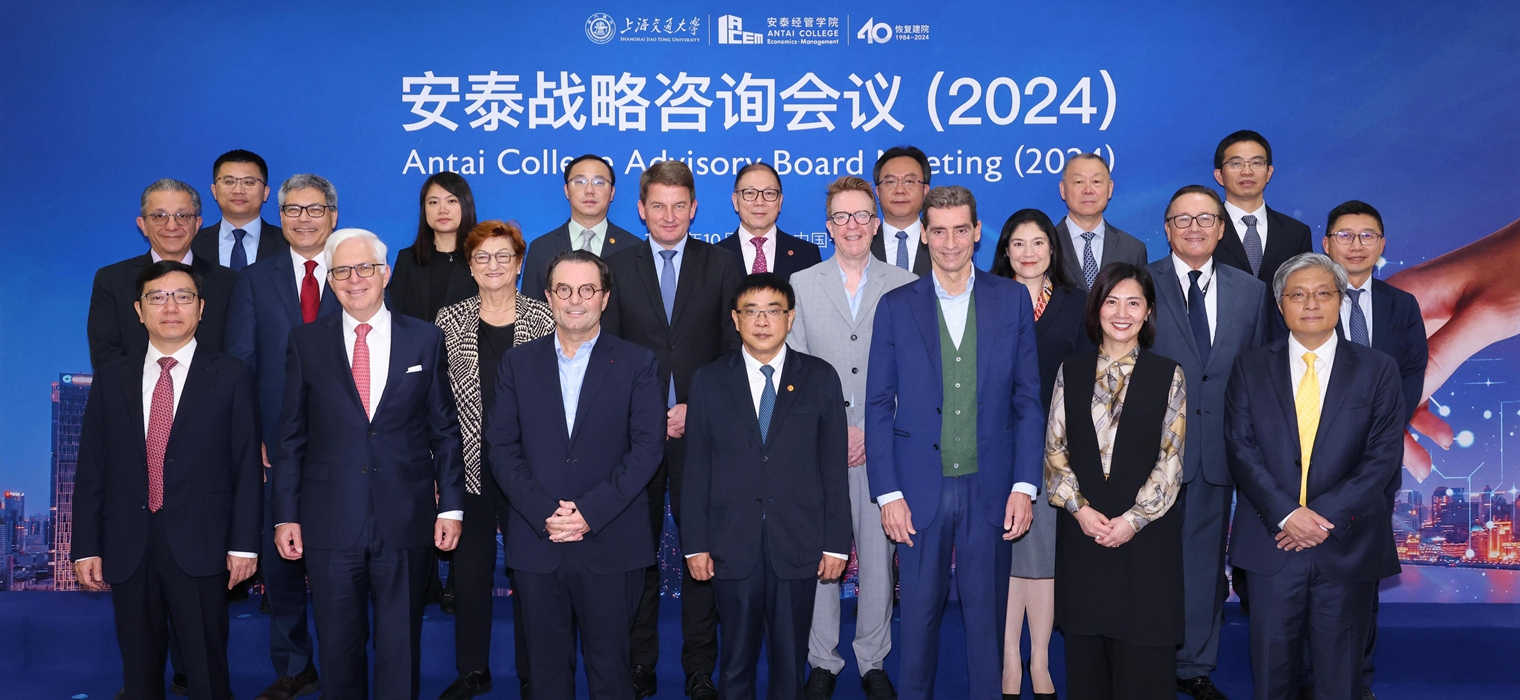
开云网页登录 安泰经济与管理学院战略咨询会议(2024)召开
海南省政协一行调研开云app官网入口下载苹果版 长兴海洋实验室
2024年10月31日
大型纪录片《李叔同》走进开云app官网入口下载苹果版 ,掀互动交流热潮
2024年11月01日
“红动沪盐”新四军革命精神进校园主题活动在开云网页登录 举办
2024年11月01日
新华网《“600号”来信》栏目进校园活动启动
2024年11月01日
开云真人app在线登录苹果
第五届亚太语料库语言学会议(APCLC 2024)在开云网页登录 召开
黄惠康教授做客开云网页登录 第155期焦点讲坛
开云网页登录 举办第二十三期青年骨干教师培训班
专家热议可持续城市更新模式,中国城市百人论坛2024秋季论坛在沪举行
技术革命与全球政治经济秩序重构——第四届“中国政治经济研究上海论坛”举办
美国计算机科学家Jon Kleinberg教授做客第230期大师讲坛